

活動名稱
【解題達人! We want you!】
活動說明
阿摩站上可謂臥虎藏龍,阿摩發出200萬顆鑽石號召達人們來解題!
針對一些題目可能有疑問但卻缺少討論,阿摩主動幫大家尋找最佳解!
懸賞試題多達20萬題,快看看是否有自己拿手的科目試題,一旦你的回應被選為最佳解,一題即可獲得10顆鑽石。
懸賞時間結束後,只要摩友觀看你的詳解,每次也會得到10顆鑽石喔!
關於鑽石
如何使用:
- ✔懸賞試題詳解
- ✔購買私人筆記
- ✔購買懸賞詳解
- ✔兌換VIP
(1000顆鑽石可換30天VIP) - ✔兌換現金
(50000顆鑽石可換NT$4,000)
如何獲得:
- ✔解答懸賞題目並被選為最佳解
- ✔撰寫私人筆記販售
- ✔撰寫詳解販售(必須超過10讚)
- ✔直接購買 (至站內商城選購)
** 所有鑽石收入,都會有10%的手續費用
近期考題
Article 6
【題組】49.__________as risk markers to improve the risk strati fication of SMI in type 2 diabetes. According to the article, which of the followings is suitable to fill in the blank?
(A) Clinical syndromes
(B) Radial pulse spectrum analysis
(C) type 2 diabetes
(D) Myocardial perfusions
(source: IEEE journal of translational engineering in health and medicine. 2018;
6:190050)
Silent Myocardial Ischemia (SMI) is an issue of public health that leads to heart
attack and significanty influences the mortality rate in patients with type 2 diabetes.
SMI is myocardial ischemia without chest discomfort and other angina symptoms. The
incidence rate of SMI in diabetic patients was 2.2 times higher than the incidence rate
of SMI in nondiabetic patients. SMI had been investigated and confirmed with a 6%-
23% prevalenco in diabetic patients using Myocardial Perfusion Imaging (MP) and
invasive coronary angiography. SMI can lead to acute myocardial infarction, adverse
cardiac events, and poor prognosis outcomes, that are severe in diabetic care. Therefore,
it is quite important to have an early predictor of SMI that can feasibly screen diabetic
patients and give a risk stratification of heart ischemia and may prevent many diabetic
patients from sudden cardiac death or adverse cardiovascular events. Holter devices,
the ambulatory clectrocardiography (ECG), has proven to be a useful tool to detect
patients at high risk of SMI. However, Holter devices need to monitor the patients over
the course of 24 hours or even up to 72 hours to detect abnormal clectrical signals from
the electrocardiogram. This long-term measurement makes the Holter less effective for
screening the whole population of high cardiovascular risk group such as diabetic
groups. Besides the ambulatory ECG, low ankle-brachial index (ABI) and
microalbuminuria, the albumin-tocreatinine ratio (ACR) between 30mg/g to 300mg/g,
have also been investigated in the detecti tion of SMI. Another potential method of
detecting SMI is using arterial pulse spectru um analysis. The spectrum of arterial pulse
wave reflects the loading condition of the arterial system, which has been investigated,
modeled, applied, and interpreted in many clinical studies. According to Lin's model,
radial pulse spectrum analysis can reveal the arterial-ventricular function by its
harmonics change. Chen et al. validated this concept and proved that the specific
characteristic of radial pulse spectrum changed from the resting state to the onset of
acute, uncomplicated myocardial infarction state, and gradually shifted to other resting
characteristics a week after surgery. Furthermore, the cross-sectional study showed that
the harmonics of the radial pulse spectrum were correlated with the ischemic heart
disease. To summarize results from those studies, the ventricular-arterial coupling
system distributed the pressure pulse wave to different organs in proportions of
harmonics according to the system state. Therefore, the pattern of harmonic
components could reveal the blood flow condition of organs, and more specifically,
reveal the condition of myocardial perfusion. However, there is still a lack of direct
statistic evidence quantifying the correlation between harmonics of the radial pulse
wave and myocardial perfusion, and validating whether the harmonics of the pulse
spectrum contains the information in identifying SMI. Hence, the objective of this study
was to statistically validate the degree of confidence that the harmonics of radial pulse
spectrum and myocardial perfusion were correlated, using receiver operating
characteristic curve (ROC) and multivariable linear regression. This report chose type
2 diabetic patients because of their high-risk prevalence for SMI. We included the
patients without any angina pectoris history, at high risk of SMI, and suitable for
performing MPI. We further investigated the relationship between SMI and different
risk factors. In the end, this report analyzed the different risk factor profiles to propose
an effective and efficient method for early SMI diagnosis.
【題組】49.__________as risk markers to improve the risk strati fication of SMI in type 2 diabetes. According to the article, which of the followings is suitable to fill in the blank?
(A) Clinical syndromes
(B) Radial pulse spectrum analysis
(C) type 2 diabetes
(D) Myocardial perfusions
Passage D: Three satellites found that 97 percent of Greenland—the land 26. second only to Antarctica for its
volume of ice—underwent a thaw never before seen in 33 years of satellite 27. , NASA reported Tuesday.
Satellite experts at first didn't trust their readings, especially since they showed an incredible 28. . Over four
days, Greenland's ice sheet—which 29. 683,000 square miles—went from 40 percent in thaw to nearly
entirely in thaw. "This was so extraordinary that at first I questioned the result: Was this real or was it 30. to a data
error?" Son Nghiem of NASA's Jet Propulsion Lab in Pasadena, Calif., said in NASA's statement about the
findings.
【題組】28.
(A)maze
(B)deflation
(C)journey
(D)acceleration
【題組】28.
(A)maze
(B)deflation
(C)journey
(D)acceleration
X 產品的產品結構圖以及物料生產(或準備)時間(PT,以天為單位)如下圖所示;
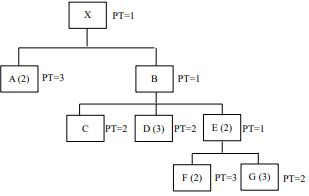
【題組】2.要生產 100 個 X,需要多少個 G?
(A)100
(B)200
(C)500
(D)600
【非選題】
【題組】 (a) The gas is expanded isothermally and reversibly until the volume triples.
5.A 3.5 mole sample of an ideal gas, for which  = 3R / 2, initially at 25℃ and 1.6x106 Pa, under goes a
two-stage transformation. For each of the stages described in the following list, calculate the final
pressure, as well as q, w, ∆U , and ∆H . Also calculate q, w, ∆U , and ∆H for the complete process.
= 3R / 2, initially at 25℃ and 1.6x106 Pa, under goes a
two-stage transformation. For each of the stages described in the following list, calculate the final
pressure, as well as q, w, ∆U , and ∆H . Also calculate q, w, ∆U , and ∆H for the complete process.
【題組】 (a) The gas is expanded isothermally and reversibly until the volume triples.