 阿摩線上測驗
阿摩線上測驗
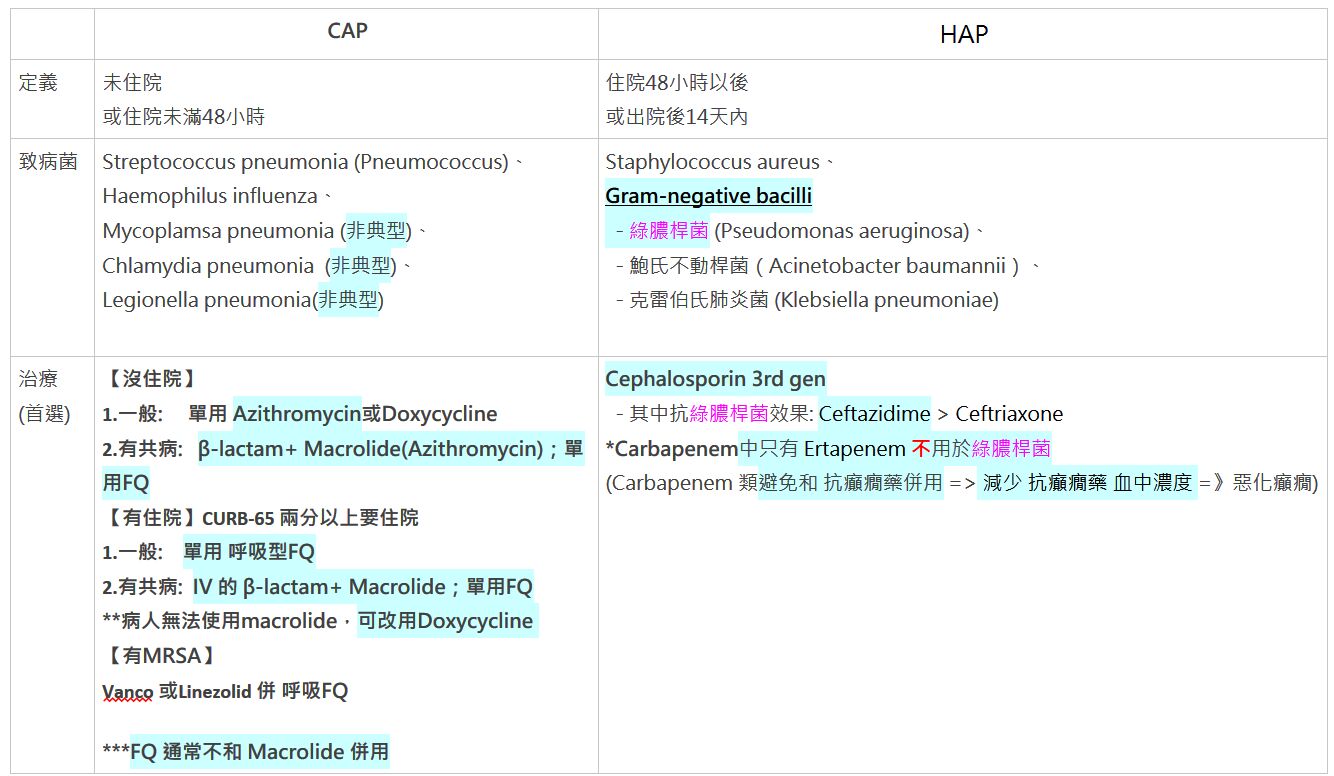
16.陳先生罹患COPD(Group C)與DM,最近2個月內發生過community acquired penumonia。這幾天其因
dyspnea、purulent sputum、痰液增多等症狀而就醫。下列empirical antibiotics何者不適當?
(A)sulfamethoxazole and trimethoprim
(B)amoxicillin and clavulanate
(C)cefuroxime
(D)levofloxacin
統計: A(2079), B(395), C(618), D(353), E(0) #3197634
詳解 (共 10 筆)
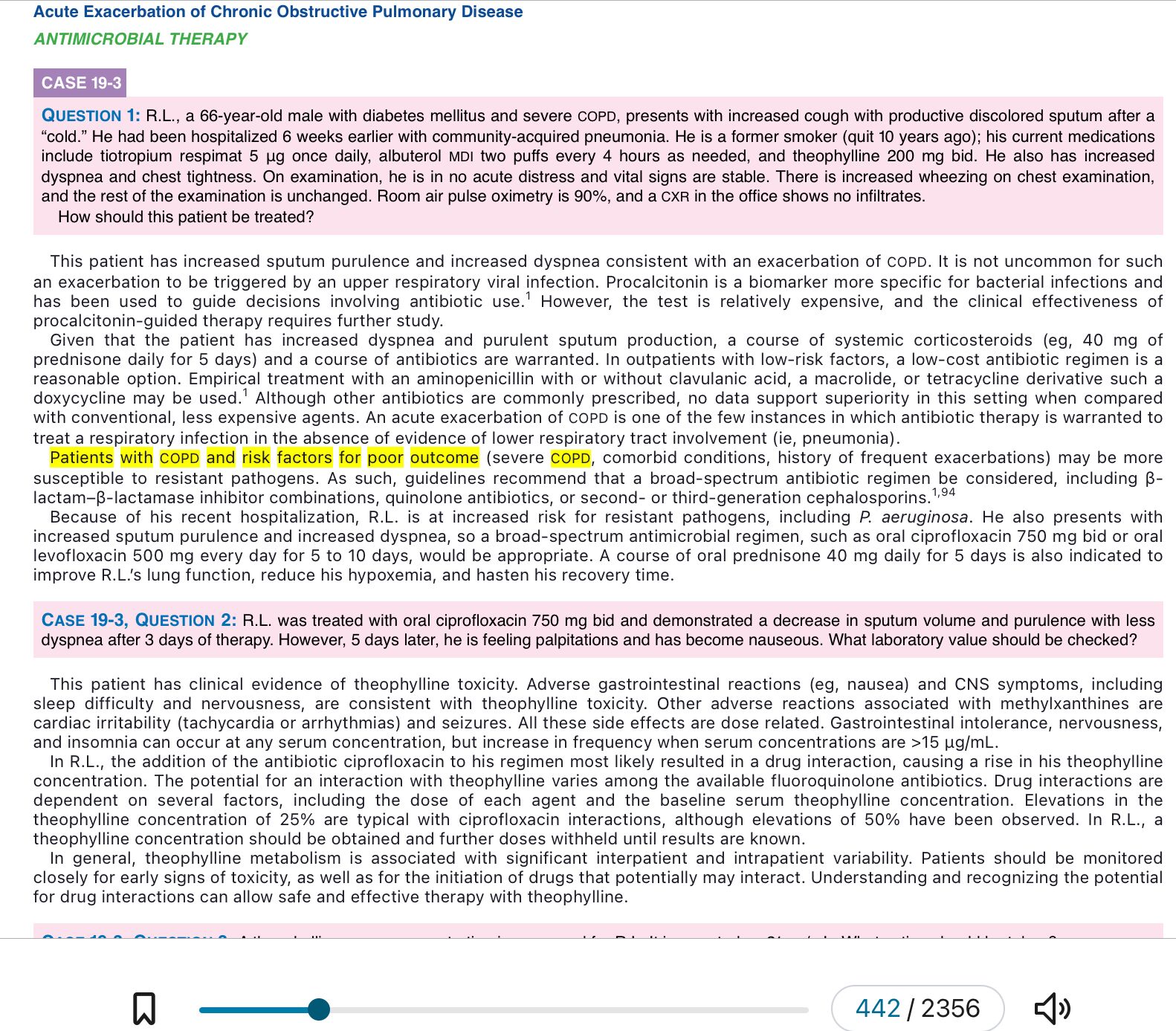
Patients with COPD and risk factors for poor outcome (severe COPD, comorbid conditions, history of frequent exacerbations) may be more susceptible to resistant pathogens. As such, guidelines recommend that a broad-spectrum antibiotic regimen be considered, including β-lactam–β-lactamase inhibitor combinations, quinolone antibiotics, or second- or third-generation cephalosporins
要選對抗生素,首先要看病人是不是「複雜型 (Complicated)」患者。這名陳先生有幾個關鍵風險因子:
-
共病症 (Comorbidities): 他有 糖尿病 (DM)。
-
近期抗生素使用史: 他最近 2 個月內 得過肺炎 (Community acquired pneumonia),暗示近期才剛吃過抗生素。
-
COPD 分級: Group C 代表症狀多或風險高。
判斷結果: 這位病人屬於 「複雜型急性惡化 (Complicated Exacerbation)」 且有抗藥性風險。
選項詳細解析
-
[(A) sulfamethoxazole and trimethoprim (Baktar)] — 不適當 (本題答案)
-
定位: 這通常是用於 「單純型 (Uncomplicated)」 的年輕病人、沒有共病症、且肺功能還不錯的人。
-
抗藥性: 在台灣,肺炎鏈球菌 (S. pneumoniae) 對 Baktar 的抗藥性相當高。
-
結論: 對於這位有糖尿病、且兩個月前才剛感染過的病人,用這個藥 太弱了,失敗率很高。
-
-
[(B) amoxicillin and clavulanate (Augmentin)] — 適當
-
定位: 這是治療複雜型 AECOPD 的 首選藥物之一。
-
優勢: 加了 Clavulanate 可以對抗會產酶的流感嗜血桿菌 (H. influenzae) 和卡他莫拉菌 (M. catarrhalis),覆蓋率足夠。
-
-
[(C) cefuroxime (Zinacef)] — 適當
-
定位: 第二代頭孢菌素 (2nd Gen Cephalosporin),也是複雜型病人的 替代選擇。
-
優勢: 抗菌範圍比第一代廣,對呼吸道常見菌種有效。
-
-
[(D) levofloxacin (Cravit)] — 適當
-
定位: 呼吸道氟奎諾酮類 (Respiratory Fluoroquinolone)。
-
優勢: 這是 最強的武器 之一。它不僅殺菌效果好,還能覆蓋非典型病原體。對於 近期用過抗生素 或 肺功能很差 的病人,這是非常標準的建議用藥。
-
藥師小筆記:AECOPD 抗生素選藥階梯
-
單純型 (年輕、沒病、久沒發作):
可以用簡單的藥,如 Amoxicillin, Doxycycline, Macrolide, 或 TMP/SMX (但在台灣因抗藥性少用)。
-
複雜型 (老人、有病、最近剛吃藥): $\leftarrow$ 陳先生在這裡
必須升級!用 Augmentin (B)、2/3代 Ceph (C)、或 Fluoroquinolone (D)。
-
綠膿桿菌風險 (住院、超爛肺功能、甚至有支氣管擴張):
一定要用 Ciprofloxacin 或 Levofloxacin (750mg) 或 抗綠膿針劑。